What Patients Should Understand About Metabolic Surgery Before Consulting a Surgeon
Overview
Metabolic surgery—often called bariatric surgery or weight loss surgery—includes procedures designed to help treat obesity and obesity-related conditions such as type 2 diabetes, high blood pressure, sleep apnea, and fatty liver disease. For some patients, surgery may be considered when lifestyle changes and medications have not led to enough improvement, or when weight-related health risks remain significant.
Before consulting a surgeon, patients should understand that metabolic surgery is not a quick fix. It is a medical treatment that requires screening, preparation, long-term nutrition changes, follow-up care, and realistic expectations. Different procedures work in different ways, and individual results vary.
This guide is educational only. It is not a diagnosis or a recommendation for surgery. A qualified clinician can help you understand whether any procedure is appropriate for your personal health history.
Key Takeaways
- Metabolic surgery includes procedures such as gastric sleeve, gastric bypass, and other bariatric operations that can affect weight, appetite, hormones, and metabolism.
- Candidacy depends on BMI, obesity-related conditions, prior treatment attempts, medical history, mental health readiness, and ability to commit to follow-up.
- Surgery carries risks, including bleeding, leaks, blood clots, nutritional deficiencies, reflux, ulcers, and the need for additional treatment.
- Recovery involves staged eating, hydration goals, activity progression, and long-term vitamin and lab monitoring.
- Patients traveling abroad should plan for medical records, travel timing, blood-clot prevention, local follow-up, and what to do if complications occur after returning home.
- Cost matters, but the safest comparison includes surgeon credentials, facility standards, anesthesia, aftercare, and emergency protocols—not price alone.
Understanding Metabolic Surgery
Metabolic surgery refers to operations that change the stomach and/or intestinal tract to help reduce food intake, alter hunger signals, and improve metabolic function. Common procedures include:
- Gastric sleeve: A large portion of the stomach is removed, creating a smaller sleeve-shaped stomach. It limits food volume and may affect hunger-related hormones. It is one of the most commonly performed bariatric procedures.
- Gastric bypass: A small stomach pouch is created and connected to part of the small intestine. This limits intake and changes how food moves through the digestive tract, with metabolic effects that may improve type 2 diabetes in some patients.
- One-anastomosis gastric bypass / mini-bypass: A variation of bypass involving one intestinal connection. It may be discussed for selected patients but has specific nutritional and reflux-related considerations.
- Revisional surgery: A follow-up procedure for patients who have had prior bariatric surgery and may have complications, weight regain, or inadequate response. Revisions are typically more complex.
Some patients researching less invasive options may also hear about endoscopic sleeve gastroplasty, which is not the same as surgical gastric sleeve. It is performed through the mouth using an endoscope and sutures rather than surgical removal of stomach tissue. It may be appropriate for some patients but has different durability, risks, and expected outcomes.
The right option depends on many factors, including BMI, diabetes status, reflux history, eating patterns, medications, prior surgeries, and willingness to follow long-term nutrition guidance.
Who It May Be For
A clinician may discuss metabolic or bariatric surgery with adults who meet guideline-based criteria. In general, candidates may include patients with:
- A BMI of 40 or higher, even without other diagnosed conditions.
- A BMI of 35 or higher with obesity-related conditions such as type 2 diabetes, hypertension, obstructive sleep apnea, or fatty liver disease.
- In some guidelines, a BMI of 30–34.9 with type 2 diabetes or metabolic disease that is not adequately controlled with nonsurgical treatment.
- A history of medically supervised attempts at weight management.
- A clear understanding that surgery requires lifelong nutrition habits, vitamin supplementation, and follow-up.
- Psychological readiness and support for major lifestyle changes.
Patients should also be medically stable enough for anesthesia and surgery. Preoperative testing may include blood work, ECG, imaging, endoscopy in selected cases, sleep apnea screening, and consultations with nutrition, psychology, cardiology, or endocrinology when appropriate.
Who Is Not a Candidate—or May Need More Preparation
Not everyone seeking weight loss surgery is an appropriate candidate at the time of consultation. Surgery may be delayed or not recommended for patients with:
- Untreated or unstable heart, lung, liver, kidney, or endocrine disease.
- Active substance use disorder or unmanaged severe mental health conditions.
- Untreated eating disorders such as active bulimia or binge-eating patterns that require stabilization.
- Inability to understand or commit to follow-up, nutrition changes, and supplementation.
- Pregnancy or plans to become pregnant soon after surgery.
- Medical conditions that make anesthesia or surgery unacceptably risky.
- Unrealistic expectations, such as expecting guaranteed weight loss or no need for long-term behavior change.
A surgeon may recommend additional evaluation, medical optimization, or nonsurgical treatment before reconsidering surgery.
Realistic Benefits Patients Should Understand
Metabolic surgery may help some patients achieve meaningful weight loss and improvement in obesity-related health conditions. Potential benefits can include:
- Reduced body weight over time.
- Improvement or remission of type 2 diabetes in some patients.
- Better blood pressure, cholesterol, sleep apnea, or fatty liver markers in selected cases.
- Improved mobility, stamina, or quality-of-life measures for some patients.
- Reduced need for certain medications, under clinician supervision.
However, outcomes vary widely. Weight loss may slow, plateau, or partially reverse. Some patients experience insufficient weight loss or weight regain. Long-term success is strongly influenced by follow-up care, nutrition, physical activity, mental health support, and management of medical conditions.
Safety Considerations and Procedure-Specific Risks
All surgery has risk. Bariatric and metabolic procedures are commonly performed, but they are still major medical treatments requiring careful screening and experienced teams.
Potential risks include:
- Bleeding or infection: May occur after surgery and sometimes requires treatment or readmission.
- Staple-line leak: A rare but serious complication after gastric sleeve or bypass-related procedures.
- Blood clots: Deep vein thrombosis or pulmonary embolism can occur after surgery, especially with long travel or limited mobility.
- Anesthesia complications: Risk varies based on health status, sleep apnea, heart or lung conditions, and medications.
- Nutritional deficiencies: Iron, vitamin B12, folate, vitamin D, calcium, and protein deficiencies can occur, especially after bypass procedures.
- Reflux or worsening GERD: Gastric sleeve may worsen reflux in some patients; a history of severe GERD should be discussed carefully.
- Dumping syndrome: More common after bypass, involving nausea, cramping, diarrhea, sweating, or dizziness after certain foods.
- Ulcers, strictures, or bowel obstruction: These may require medication, endoscopy, or additional procedures.
- Gallstones: Rapid weight loss can increase gallstone risk.
- Mental health changes: Mood, body image, alcohol sensitivity, and eating behaviors can shift after surgery.
Ask how the surgical team screens for these risks, what emergency plans are in place, and how complications are managed if you return home.
Travel Planning for Patients Considering Care Abroad
Many US and Canadian patients research bariatric surgery abroad because of access, cost, or wait-time concerns. Travel adds planning considerations beyond the procedure itself.
Before booking travel, patients should ask for:
- Surgeon credentials, training, board certification or equivalent qualifications, and experience with your procedure.
- Facility accreditation or licensing information.
- Anesthesia team qualifications.
- Clear preoperative testing requirements.
- Written discharge instructions in English.
- Copies of operative reports, lab results, medication lists, and imaging reports in English.
- A plan for follow-up with your primary care clinician or bariatric team at home.
Blood-Clot Precautions During Travel
Long flights or car rides can increase clot risk after surgery. Discuss prevention with your clinical team. General precautions may include:
- Walking frequently during travel when cleared.
- Flexing ankles and calves while seated.
- Staying hydrated as instructed.
- Avoiding unnecessary prolonged immobility.
- Using compression stockings if recommended.
- Taking blood-thinning medication only if prescribed.
Do not self-prescribe aspirin, anticoagulants, or supplements without medical guidance.
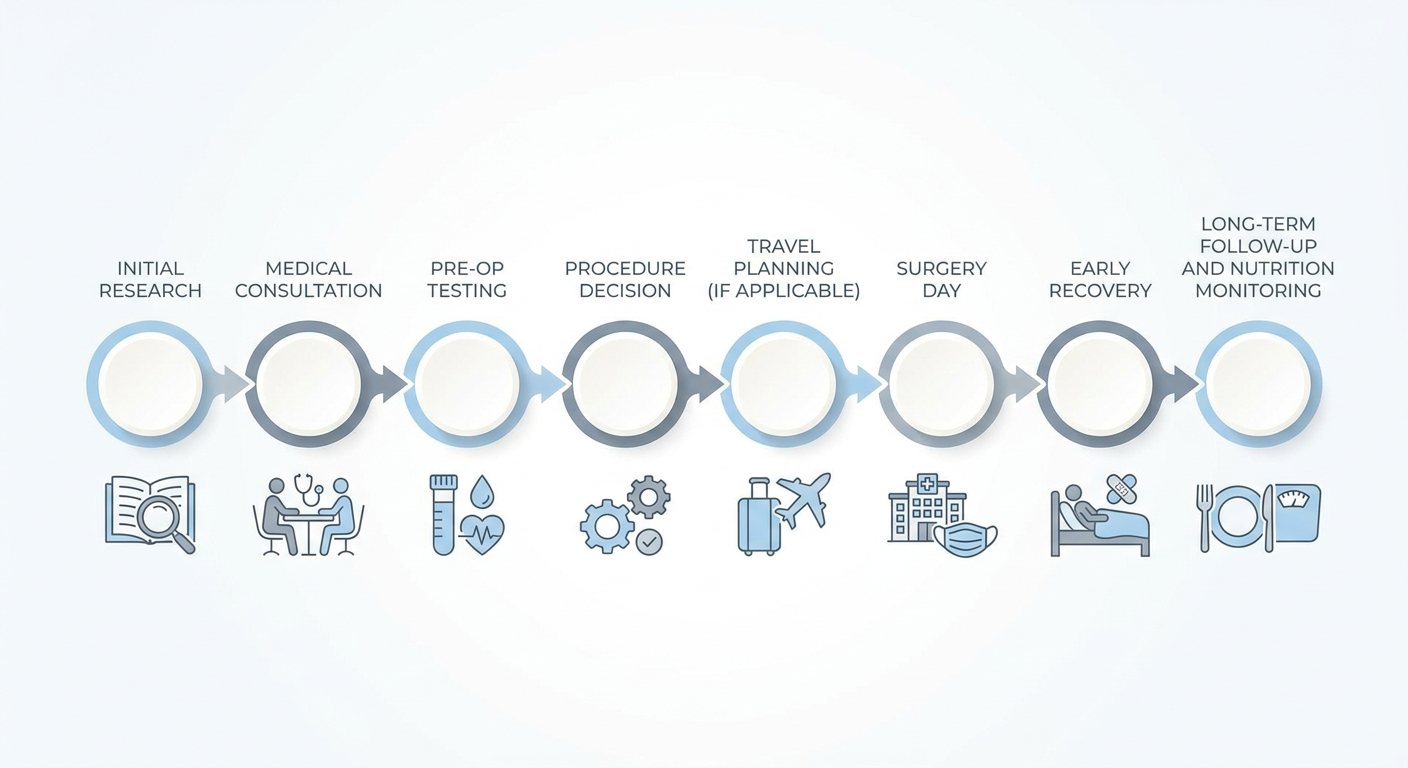
Recovery / What to Expect
Recovery varies by procedure and patient health status, but many programs follow a staged plan.
First days: Patients are monitored for hydration, pain control, nausea, breathing, walking tolerance, and signs of complications. Many patients start with clear liquids.
Weeks 1–2: Focus is usually on hydration, protein goals, walking, rest, and following the prescribed liquid or puréed diet. Fatigue is common. Patients should watch for fever, increasing abdominal pain, shortness of breath, chest pain, repeated vomiting, calf swelling, or inability to keep fluids down.
Weeks 3–6: Food texture often advances gradually, depending on the program. Light activity usually increases. Heavy lifting and strenuous exercise may still be restricted until cleared.
Months 2–12: Weight loss often progresses, but the pace varies. Lab monitoring, vitamin supplementation, protein intake, strength-building activity, and medical follow-up become central.
Long term: Bariatric surgery requires ongoing care. Patients may need annual labs, nutritional supplementation, medication adjustments, pregnancy planning guidance, and support for weight maintenance.
Cost Context
Costs vary by country, city, facility, procedure type, medical complexity, and what is included. In the US and Canada, insurance coverage, public wait times, deductibles, and eligibility requirements can vary widely. Self-pay bariatric surgery in the US may cost significantly more than in some medical travel destinations.
In Mexico and other international destinations, package pricing for procedures such as gastric sleeve may sometimes be lower than US self-pay prices. However, patients should avoid comparing quotes based on price alone. Ask what is included: surgeon fee, anesthesia, hospital stay, pre-op testing, medications, hotel, transportation, complication management, and follow-up access. Also consider travel costs, time off work, caregiver support, and the possibility of needing care after returning home.
No clinic can responsibly promise a total cost for every patient before reviewing medical history and testing.
Questions to Ask a Clinician
Bring a written checklist to your consultation:
- Which procedure do you recommend for me, and why?
- What alternatives should I consider, including medication or endoscopic options?
- How does my BMI, diabetes status, reflux history, and prior surgery history affect the recommendation?
- What are my personal risk factors for complications?
- How many of this procedure have you performed?
- What is the facility’s accreditation or licensing status?
- Who provides anesthesia, and what are their qualifications?
- What preoperative tests are required?
- What is the plan if a leak, bleeding, clot, or infection occurs?
- How long should I stay near the surgical facility before traveling home?
- What diet stages will I follow after surgery?
- Which vitamins and labs will I need long term?
- How will you coordinate with my doctor at home?
- What costs are included, and what costs are not included?
FAQ
Is metabolic surgery the same as weight loss surgery?
The terms overlap. “Weight loss surgery” emphasizes weight reduction, while “metabolic surgery” highlights effects on obesity-related diseases such as type 2 diabetes. Procedures such as gastric sleeve and gastric bypass are often considered both bariatric and metabolic.
How much weight will I lose?
Weight loss varies by procedure, starting weight, health conditions, diet, activity, medications, and follow-up. A clinician can discuss typical ranges, but no result is guaranteed.
Is gastric sleeve safer than gastric bypass?
Neither procedure is automatically “safer” for every patient. Gastric sleeve and bypass have different risk profiles. For example, sleeve may be a concern for patients with severe reflux, while bypass may carry higher nutritional monitoring needs. Your history matters.
Can surgery improve type 2 diabetes?
Some patients experience significant improvement in blood sugar control after metabolic surgery, and some may reduce medications under medical supervision. Results vary, and long-term monitoring remains important.
How soon can I fly after bariatric surgery?
Timing depends on the procedure, your recovery, clot risk, and surgeon guidance. Patients traveling abroad should discuss how long to remain near the surgical facility and how to reduce travel-related clot risks.
Will I need vitamins forever?
Many bariatric patients require lifelong supplementation, especially after bypass procedures. Your care team should provide a specific plan for vitamins, minerals, protein intake, and lab monitoring.
What records should I bring home after surgery abroad?
Ask for your operative report, discharge summary, medication list, lab results, imaging reports, complication notes if applicable, and nutrition instructions in English. Share these with your clinician at home.
Next Steps
If you are considering metabolic or bariatric surgery, start by gathering your medical history, medication list, prior weight management attempts, recent lab results, and questions. A qualified clinician can review your personal risks, explain procedure options, and help determine whether surgery—or another treatment path—may be appropriate.
To learn whether you may be a candidate, you may request a private consultation with a qualified clinician. The goal is education, safety, and informed decision-making—not pressure.
Medical Disclaimer
This article is for educational purposes only and does not provide medical advice, diagnosis, or treatment. Metabolic and bariatric surgery decisions should be made with a qualified healthcare professional who can evaluate your individual medical history. Individual results and risks vary.
Sources
- American Society for Metabolic and Bariatric Surgery. Patient learning resources and metabolic/bariatric surgery information.
- International Federation for the Surgery of Obesity and Metabolic Disorders. Guidelines and position statements on bariatric and metabolic surgery.
- National Institute of Diabetes and Digestive and Kidney Diseases. Weight-loss surgery information for patients.
- Obesity Canada. Clinical practice guideline resources on obesity management.
- Centers for Disease Control and Prevention. Travel-associated venous thromboembolism information.
Schema.org Recommendations
Recommended structured data for this article:
- Article schema with headline, description, author/reviewer, datePublished, dateModified, and medical disclaimer.
- MedicalWebPage schema to indicate medically oriented educational content.
- FAQPage schema for the FAQ section.
- BreadcrumbList schema for site navigation.
- ImageObject schema for the hero image and infographic if published.