How Gastric Sleeve, Bypass, and Mini-Bypass Differ in Mechanism
Overview
Patients researching bariatric surgery often compare three common procedures: gastric sleeve, gastric bypass, and mini-bypass. They may sound similar because all are designed to support weight loss and metabolic improvement, but they work in different ways.
The main differences involve how the stomach is reshaped, whether the intestines are rerouted, and how the procedure affects appetite, fullness, reflux, blood sugar regulation, and nutrient absorption. Understanding the mechanism can help you have a more informed conversation with a qualified bariatric surgeon—especially if you are comparing options in the US, Canada, or abroad.
This article is educational and does not determine which procedure is right for you. Individual risks and results vary, and a personal recommendation should come from a qualified clinician who can review your medical history, medications, labs, weight history, and goals.
Key Takeaways
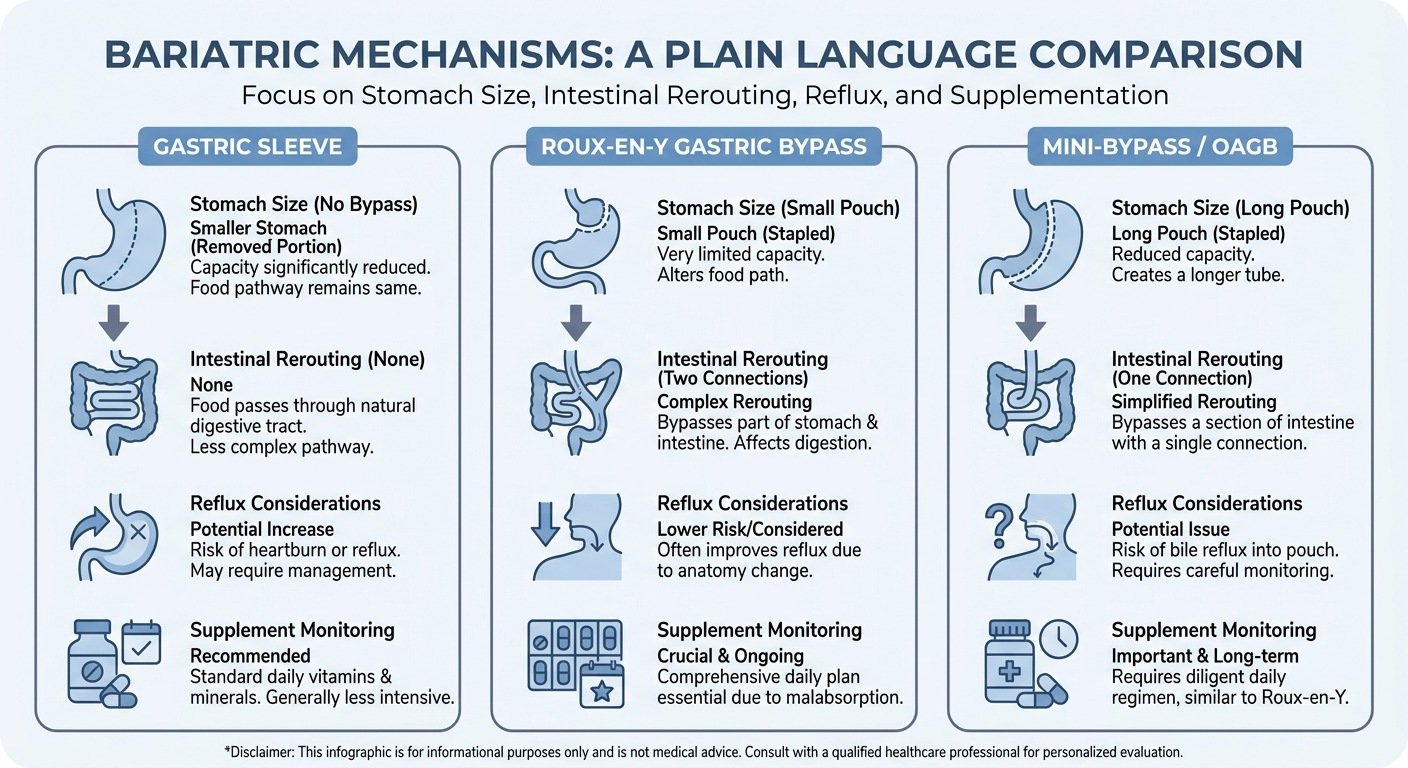
- Gastric sleeve reduces stomach size but does not bypass the intestines.
- Gastric bypass creates a small stomach pouch and reroutes part of the small intestine.
- Mini-bypass, also called one-anastomosis gastric bypass, uses a longer stomach pouch and a single connection to the small intestine.
- Each option has different effects on reflux, diabetes, nutrition, and long-term follow-up needs.
- Travel for surgery requires planning for records, follow-up, hydration, and blood-clot prevention.
- No procedure guarantees a specific amount of weight loss or metabolic improvement.
Understanding the Procedures: How They Work
Gastric sleeve: smaller stomach, no intestinal bypass
A gastric sleeve, or sleeve gastrectomy, removes a large portion of the stomach and reshapes the remaining stomach into a narrow sleeve. Food still follows the usual route: esophagus → stomach → small intestine.
Mechanisms include:
- Restriction: The smaller stomach holds less food, so patients often feel full sooner.
- Appetite hormone changes: The removed portion includes areas involved in ghrelin production, a hormone associated with hunger. Appetite changes vary by person.
- Faster stomach emptying: Some patients experience changes in how food moves through the stomach, which may affect fullness and blood sugar patterns.
Because the intestines are not bypassed, sleeve surgery generally has less malabsorption than bypass procedures. However, vitamin and mineral supplementation is still important.
One key consideration: sleeve can worsen or contribute to gastroesophageal reflux disease (GERD) in some patients. People with severe reflux or Barrett’s esophagus need careful evaluation.
Gastric bypass: small pouch plus intestinal rerouting
The most established form of gastric bypass is the Roux-en-Y gastric bypass. In this operation, the surgeon creates a small stomach pouch and connects it to a lower part of the small intestine. Food bypasses most of the stomach, the duodenum, and part of the jejunum.
Mechanisms include:
- Restriction: The small pouch limits the amount of food that can be comfortably eaten at one time.
- Hormonal and metabolic effects: Rerouting food changes gut hormone signaling, which can improve blood sugar control in some patients.
- Reduced absorption: Some calories and nutrients may be absorbed differently because food skips part of the upper intestine.
- Dumping physiology: Sugary or high-fat foods may move quickly into the small intestine, causing nausea, cramping, sweating, diarrhea, or rapid heartbeat in some patients.
Gastric bypass is often discussed for patients with obesity and type 2 diabetes, and it may be considered in some patients with significant reflux. It also requires lifelong attention to vitamins, minerals, protein intake, and follow-up labs.
Mini-bypass: one connection, longer bypassed segment
The term mini-bypass usually refers to one-anastomosis gastric bypass (OAGB). It creates a long, narrow stomach pouch and connects it to the small intestine using one surgical connection rather than the two connections used in Roux-en-Y gastric bypass.
Mechanisms include:
- Restriction: The long pouch limits meal size.
- Intestinal bypass: Food bypasses part of the small intestine, which can affect nutrient absorption.
- Metabolic hormone changes: Like other bypass procedures, it can influence gut hormones involved in appetite and blood sugar.
Potential advantages discussed in surgical literature include technical simplicity and strong metabolic effects for selected patients. However, mini-bypass may carry concerns about bile reflux, nutritional deficiencies, and the importance of experienced surgical technique and long-term monitoring. It is not the same operation as sleeve or Roux-en-Y bypass, and terminology can vary by clinic, so patients should ask exactly what anatomy is being created.
Who It May Be For
Bariatric procedures may be considered for adults with obesity when non-surgical efforts have not led to sufficient or durable improvement and when the benefits may outweigh the risks. Candidacy often depends on BMI, obesity-related conditions, prior surgery, reflux history, diabetes status, eating patterns, medications, mental health, and ability to participate in follow-up.
A clinician may discuss bariatric surgery with patients who have:
- A BMI in a range where surgery is supported by current guidelines.
- Obesity-related conditions such as type 2 diabetes, sleep apnea, hypertension, fatty liver disease, or joint disease.
- A history of weight regain after structured medical weight management.
- Readiness for nutrition changes, supplements, follow-up labs, and long-term lifestyle support.
Procedure selection is individualized. For example, a patient with severe reflux may be counseled differently than a patient without reflux. A patient with diabetes may have different priorities than someone primarily concerned about GERD symptoms or medication absorption.
Who Is Not a Candidate—or May Need More Evaluation
A person may not be ready for bariatric surgery, or may need additional evaluation first, if they have:
- Untreated or unstable severe psychiatric illness.
- Active substance use disorder.
- Inability to follow nutrition, hydration, medication, or follow-up instructions.
- Untreated eating disorder behaviors that need specialized care first.
- Medical conditions that make anesthesia or abdominal surgery unusually high risk.
- Pregnancy or plans for pregnancy in the near term.
- Severe reflux or esophageal disease that may make sleeve less appropriate.
- Prior abdominal surgery or anatomy that requires specialized planning.
This is not a complete list. A qualified bariatric team should review your individual risks.
Realistic Benefits
Potential benefits may include weight loss, improved mobility, reduced medication needs, and improvement in obesity-related conditions such as type 2 diabetes, sleep apnea, high blood pressure, and fatty liver disease. Some patients experience improved quality of life, energy, and ability to participate in physical activity.
However, outcomes vary. Surgery is not a stand-alone cure. Long-term results depend on the procedure, biology, follow-up care, nutrition, physical activity, mental health support, and management of weight regain risks.
Safety Considerations and Procedure-Specific Risks
All bariatric operations carry risks related to anesthesia, bleeding, infection, blood clots, leaks, dehydration, nausea, vomiting, strictures, gallstones, and the need for additional procedures. Risks can be reduced—but not eliminated—by careful patient selection, an experienced team, accredited facilities, and appropriate follow-up.
Procedure-specific considerations include:
Gastric sleeve risks
- Staple-line leak or bleeding.
- New or worsened GERD.
- Narrowing or twisting of the sleeve.
- Nausea, vomiting, or intolerance of certain foods.
- Long-term vitamin and mineral deficiencies, though usually less malabsorptive than bypass.
Gastric bypass risks
- Leak or bleeding at surgical connections.
- Marginal ulcers, especially with smoking or NSAID use.
- Internal hernia or bowel obstruction.
- Dumping syndrome.
- Greater need for lifelong supplementation and lab monitoring.
- Medication absorption changes.
Mini-bypass risks
- Leak or bleeding at the single connection.
- Bile reflux into the stomach pouch or esophagus.
- Protein-calorie malnutrition or micronutrient deficiencies if absorption is significantly affected.
- Ulcers, diarrhea, or food intolerance.
- Need for long-term follow-up with a team familiar with OAGB anatomy.
Ask your surgeon how they screen for reflux, diabetes, nutritional risk, and prior abdominal conditions before recommending one procedure over another.
Travel Planning for Surgery Abroad
If you are considering bariatric care outside your home country, planning should focus on safety, continuity, and documentation—not just price.
Before travel, request:
- A written surgical plan explaining the exact procedure and anatomy.
- Surgeon credentials, facility accreditation, and emergency protocols.
- Pre-op testing requirements and medication instructions.
- A plan for communication with your primary care clinician at home.
- English-language medical records, including operative report, discharge summary, lab results, and medication list.
Blood-clot precautions
Long flights or car rides after surgery can increase the risk of venous thromboembolism. Ask your clinician about:
- When it is safe to fly or travel by car.
- Compression stockings.
- Walking breaks during travel.
- Hydration goals.
- Whether blood-thinning medication is appropriate for your risk profile.
- Warning signs such as calf swelling, chest pain, or shortness of breath.
Do not self-start blood thinners or supplements without clinician guidance.
Recovery / What to Expect
Recovery timelines vary, but many patients follow a staged approach:
- First 24–48 hours: Monitoring for pain control, hydration, nausea, walking, and early complications.
- Week 1: Clear or full liquid diet, frequent sipping, short walks, and avoiding lifting. Fatigue is common.
- Weeks 2–4: Gradual transition through pureed or soft foods depending on the program. Focus on protein, hydration, and supplements.
- Weeks 4–6: Many patients return to routine daily activities, though strenuous exercise may still be limited until cleared.
- Months 2–12: Ongoing weight loss, diet progression, lab monitoring, and attention to hair shedding, constipation, reflux, dumping symptoms, or food intolerance.
- Long term: Annual labs, supplements, weight maintenance strategies, and support for nutrition, movement, and mental health.
Bypass and mini-bypass patients often need especially careful monitoring of iron, B12, folate, vitamin D, calcium, thiamine, and protein status. Sleeve patients also need supplementation and labs, even without intestinal bypass.
Cost Context
Costs vary widely by country, facility, surgeon, testing needs, travel, and aftercare. In the US, bariatric surgery may range from roughly $15,000–$30,000+ USD without insurance, though insurance coverage may apply. In Canada, private-pay options and wait times vary by province and program. International self-pay packages may sometimes be quoted in the $4,000–$10,000+ USD range, but inclusions differ significantly.
When comparing costs, ask what is included: hospital fees, anesthesia, surgeon fees, pre-op testing, hotel, transportation, medications, complication care, and follow-up. A lower quote is not automatically safer or riskier; the key is transparency, credentials, facility standards, and continuity of care.
Questions to Ask a Clinician
Bring this checklist to your consultation:
- Which procedure are you recommending for me, and why?
- How do my reflux history, diabetes status, medications, and labs affect the choice?
- For mini-bypass, exactly how much intestine is bypassed?
- What are your leak, complication, and readmission protocols?
- What facility will be used, and what emergency resources are available?
- What pre-op testing do I need?
- What diet stages and supplements will I follow?
- How will I get English-language medical records?
- Who handles follow-up after I return home?
- What symptoms should prompt urgent care?
- How do you monitor for nutritional deficiencies over time?
FAQ
Is gastric sleeve safer than bypass?
Safety depends on the individual patient, the surgical team, and the facility. Sleeve avoids intestinal rerouting but may worsen reflux. Bypass has more complex anatomy and nutritional considerations but may be preferable for some patients with reflux or metabolic disease.
Does bypass cause more weight loss than sleeve?
Some studies show greater average weight loss or metabolic effects with bypass procedures, but individual results vary. Long-term habits, biology, follow-up, and complications all matter.
Is mini-bypass the same as gastric bypass?
No. Mini-bypass, or one-anastomosis gastric bypass, uses one intestinal connection and creates different anatomy than Roux-en-Y gastric bypass. Ask your surgeon to draw or explain the planned anatomy.
Which procedure is better for acid reflux?
It depends on the cause and severity of reflux. Sleeve may worsen GERD in some patients, while Roux-en-Y bypass may improve reflux for selected patients. Mini-bypass requires careful discussion because bile reflux can be a concern.
Will I need vitamins forever?
Most bariatric programs recommend lifelong supplementation and periodic lab monitoring after any bariatric procedure. This is especially important after bypass and mini-bypass.
How soon can I fly after surgery?
Timing varies by your risk factors and surgeon’s protocol. Ask about clot prevention, hydration, walking, compression stockings, and whether you need medication to reduce clot risk.
Can these procedures be reversed?
Sleeve is not reversible because part of the stomach is removed. Some bypass procedures may be revised in specific circumstances, but revision surgery can be complex and carries risks.
Next Steps
If you are comparing gastric sleeve, gastric bypass, and mini-bypass, focus on mechanism, safety, long-term follow-up, and how each option fits your health history. A qualified bariatric clinician can help you understand which approach—if any—may be appropriate for you.
To explore your options in a calm, private setting, you may request a consultation with a qualified clinician who can review your history, answer your questions, and explain realistic next steps.
Medical Disclaimer
This article is for educational purposes only and is not medical advice, diagnosis, or treatment. Bariatric surgery decisions should be made with a qualified healthcare professional who can evaluate your individual health status. Outcomes, risks, recovery, and weight-loss results vary.
Sources
- American Society for Metabolic and Bariatric Surgery (ASMBS): Patient learning resources and bariatric procedure information.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Weight-loss surgery overview.
- International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Bariatric and metabolic surgery guidance.
- Enhanced Recovery After Surgery (ERAS) Society: Perioperative care principles for bariatric surgery.
- Centers for Disease Control and Prevention (CDC): Travel health and blood clot prevention guidance.
Schema.org Recommendations
Recommended structured data for this article:
MedicalWebPagefor the main article page.MedicalProcedurefor gastric sleeve, Roux-en-Y gastric bypass, and one-anastomosis gastric bypass references.FAQPagefor the FAQ section.BreadcrumbListfor site navigation.OrganizationandWebSiteschema for Endoscopic Sleeve Guide.